Shoulder Impingement Syndrome
What is it?
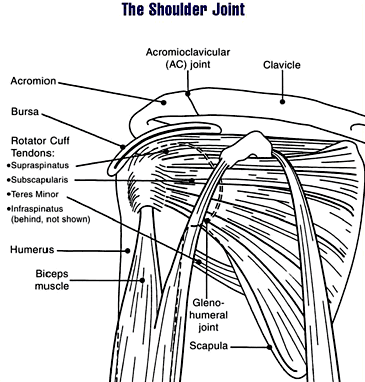
- Injury to the rotator cuff tendon(s) when there is narrowing between the head of the humerus and the coraco-acromial arch (the arcomion & the coracoacromial ligament attaching to the coracoid process) thus causing subacromial crowding. [1,2,3,4]
- Resulting in micro trauma, ischemia, swelling / inflammation further impingement
- Primarily affects the supraspinatus tendon but can also affect the infraspinatus[1,2,3]
Causes of Subacromial Crowding[1,2,3,4]
Congenital Variations
- Size or shape of the coracoid or acromion processes (boney areas)
- Coracoacromial ligament / subacromial bursal thickness
- Degree of mid-back ‘thoracic’ kyphosis; excessive curve further facilitates rounding of the shoulder blade ‘scapula’ thus decreasing subacromial space
Developmental or degenerative Factors
- Post traumatic / post surgical rotator cuff scarring
- Post trauma ‘sprain’ of acromialclavicular joint separation, laxity in ligaments
- Osteophyte formation
- Calcium deposit in rotator cuff tendon
Traumatic factors
- Disruption of ligament, cartilage and rotator cuff or biceps tendons in shoulder
- Shoulder subluxation / dislocation
Biomechanical factors
- Weakness of depressors of glenohumeral head (rotator cuff muscles) due to nerve injury or disuse
- Capsular restriction due to tightness / adhesions
- Weakness of shoulder blade muscle stabilizers altering alignment / movement
- Rotator cuff muscle imbalance
- Adhesive capsulitis ‘frozen shoulder’
Classification of impingement in 3 stages[1,8]
Stage 1
- Any age: (usually under 30 years) repetitive shoulder use “overhead athletes”
- Reversible rotator cuff injury
- Local tenderness to palpation
- Restricted range of motion and weakness
- Tendinosis / tendinopathy of rotator cuff tendon which can become fibrotic
Stage 2
- Usually 30 to 40 years of age
- Pathology not reversible by time or / and modifying activity alone
- Local tenderness to palpation and with movement, crepitus with movement
- Loss of active & passive range of motion
Stage 3
- Usually greater than 40 years
- Some degree of irreversible pathology
- Continued increase pain on palpation and with movement
- Loss of active range of motion greater than passive motion
- Atrophy ‘loss in size’ of rotator cuff and shoulder musculature
Signs & Symptoms to look out for[1,2,3,4,8]
- Pain in lateral upper arm, deltoid insertion, subacromial area (below boney process)
- Can be from repetitive arm, shoulder use (athletics: tennis, swimming, throwing overhead, computer use, overhead motion)
- Inability to lower arm from 90 degrees slowly or smoothly with or without pain
- Painful arc: catching of swollen rotator cuff tendon(s) or bursa
Other Possible Diagnosis[1,2,3.4]
- Torn labrum (cartilage)
- Instability (due to torn ligament)
- Rotator cuff / Long head Biceps tendonitis, Bursitis
- Cervical (neck) pathology: disc / nerve root
- Adhesive Capsulitis (Frozen Shoulder)
Treatment & Management
Research studies, using randomized control trials, reveal that treatments consisting of manual therapy, using joint mobilizations, and specific prescribed Physiotherapy exercises are most effective for recovery versus strengthening exercises alone.[3,5,6] Treatments are aimed towards restoring joint alignment and mobility by breaking up joint capsule restrictions (scar tissue) and correcting muscle imbalances and kinesthetic & proprioceptive awareness.[5,6] Activity modification can also aid in the management of or / and further prevention of the pathology from occurring.
The use of non-corticosteroid medication & corticosteroid injections has a role in the treatment of inflammation and pain control.[7]
When conservative treatment fails and the shoulder impingement is causing considerable pain & dysfunction, arthroscopic surgery followed by manual therapy and exercise has shown to be effective.[8]
For more information about shoulder impingement or shoulder injuries please contact InSync Physio.
References
- ^ Pyne. Diagnosis and Current Treatment Options of Shoulder Impingement. Current Sports Medicine Reports. 251 - 255, 2004 March.
- ^ Fu et al. Shoulder Impingement: A critical review. Clinical Orthopaedics and Related Research. 269: 162 – 173, 1991 August.
- ^ Kamkar et al. Nonoperative Management of Secondary Impingement Syndrome. Journal of Orthopaedics and Sports Physical Therapy. 17(5): 212 – 224, 1993 May.
- ^ Payne et al. The Combined Dynamic & Static Contributions to Subacromial Impingement: A Biomechanical Analysis. The American Journal of Sports Medicine. 25 (6): 801 – 808. 1997.
- ^ Senbursa et al. Comparison of Conservative Treatment with & without Physical Therapy for patients with Impingement Syndrome: A prospective, randomized clinical trial. Knee Surgery, Sports Traumatology, Arthroscopy. 15(7): 915 – 921. 2007.
- ^ Bang et al. Comparison of Supervised Exercise with & without Manual Physical Therapy for patients with Shoulder Impingement Syndrome. The Journal of Orthopaedic and Sports Physical Therapy. 30(3): 126 – 137. 2000.
- ^ Akgun et al. Is Local Subacromial Corticosteroid Injection Beneficial in Subacromial Impingement Syndrome? Clinical Rheumatology. 23(6): 496 – 500. 2004.
- ^ Brox et al. Arthroscopic Surgery versus Supervised Exercises in patients with rotator cuff disease (stage 2 impingement syndrome): A Prospective, randomized, controlled study in 125 patients with a 2-½ year follow-up. Journal of Shoulder and Elbow Surgery. 8(2): 102 – 111. 1999.